CASE DETAILS- A 20 yrs female with lower abdominal pain
 Fig 4 - Photograh showing per operative view of pelvic cyst
Fig 4 - Photograh showing per operative view of pelvic cyst
 Fig 5- Post op gross specimen showing ectocyst layer ( red piece) , endocyst layer( creamy white piece) , & multiple small daughter cysts in kidney tray .
Fig 5- Post op gross specimen showing ectocyst layer ( red piece) , endocyst layer( creamy white piece) , & multiple small daughter cysts in kidney tray .
AT US - A large well defined rounded complex multicystic mass noted in pelvis separate from normally appearing uterus and ovaries. The mass was harbouring multiple small rounded cysts ranging10 to 20 mm in size , mostly similar, like bunch of grapes, with echofree interior . The lesion was seen superior & slightly right to uterus and bladder. No internal echos or vascularity noted within mass . The mass was showing slight double layered mural appearance at periphery. No solid components seen . No free fluid was noted in POD. No calcific foci or any other internal complexity was appreciated . No any other similar lesion was seen elsewhere in abdomen. On the basis of US findings a diagnosis of benign complex pelvic cyst , possibly Hydatid cyst of right broad ligament [ primary pelvic peritoneal hydatid disease ], was made. Which was confirmed at surgery.


Fig 2 - TVS scan showing double layered peripheral wall of the multicystic mass
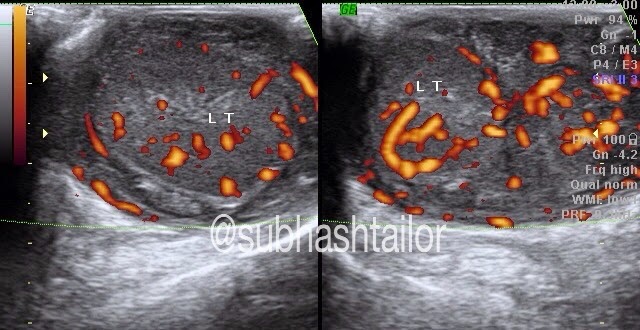
 Fig 3 - TVS scans showing normally & separately appearing uterus & both ovaries
Fig 3 - TVS scans showing normally & separately appearing uterus & both ovaries
Fig 1- TVS scan showing a large complex multicystic pelvic mass with multiple rounded daughter cysts in it, & the mass was separate from uterus & both ovaries
AT SURGERY- Rt broad ligament Hydatid cyst with thin filmy adhesion with right ovary, bladder wall, adjacent bowel loops & abdominal wall noted . The cyst was successfully operated and removed.
PS- 1) The case study is intended for medical professionals & imaging specialists for academic interests.
2) Special thanks to Dr S P sharma ( Surgeon, Bhilwara (raj, India) for operative feedback.